RTI case forces Manipur to disclose district-wise IDP data: 43,000 displaced, 731 dead, 25 unnatural deaths, and 217 terminal illness cases in Imphal East since May 2023.
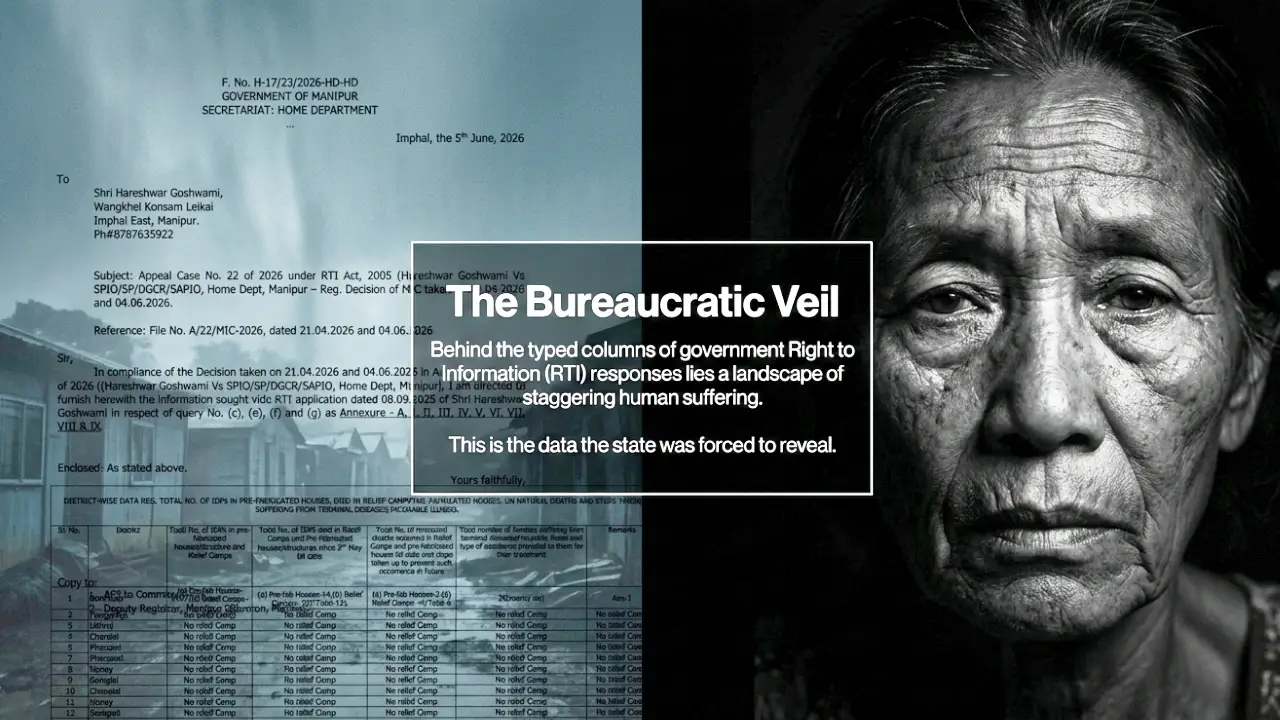
Imphal, June 7: More than 43,000 people remain displaced in Manipur's relief camps and pre-fabricated housing colonies, with 731 deaths recorded among them in the three years since the violence of May 3, 2023 first drove communities from their homes. The figures — district by district, death by death — were released last week by the state Home Department, not voluntarily, but at the end of a nine-month legal process that required two rounds of RTI proceedings, a commission directive, and a formal apology from the government for delays.
The data was finally furnished on June 5 by Joint Secretary (Home) Moirangthem Kapajit Singh in compliance with RTI Appeal Case No. 22 of 2026. The man who forced it into the open was Shri Hareshwar Goshwami, who filed his original application on September 8, 2025. What followed was a slow grind through administrative resistance — non-supply of information, a second appeal, intervention by the Manipur Information Commission — before the state produced what is now the most detailed public accounting of its displaced population since the crisis began.
The Scale: Who Is Where, and How Many
The displacement is not spread evenly across the state. Three districts bear the overwhelming weight of the crisis, and within those, the numbers are stark.
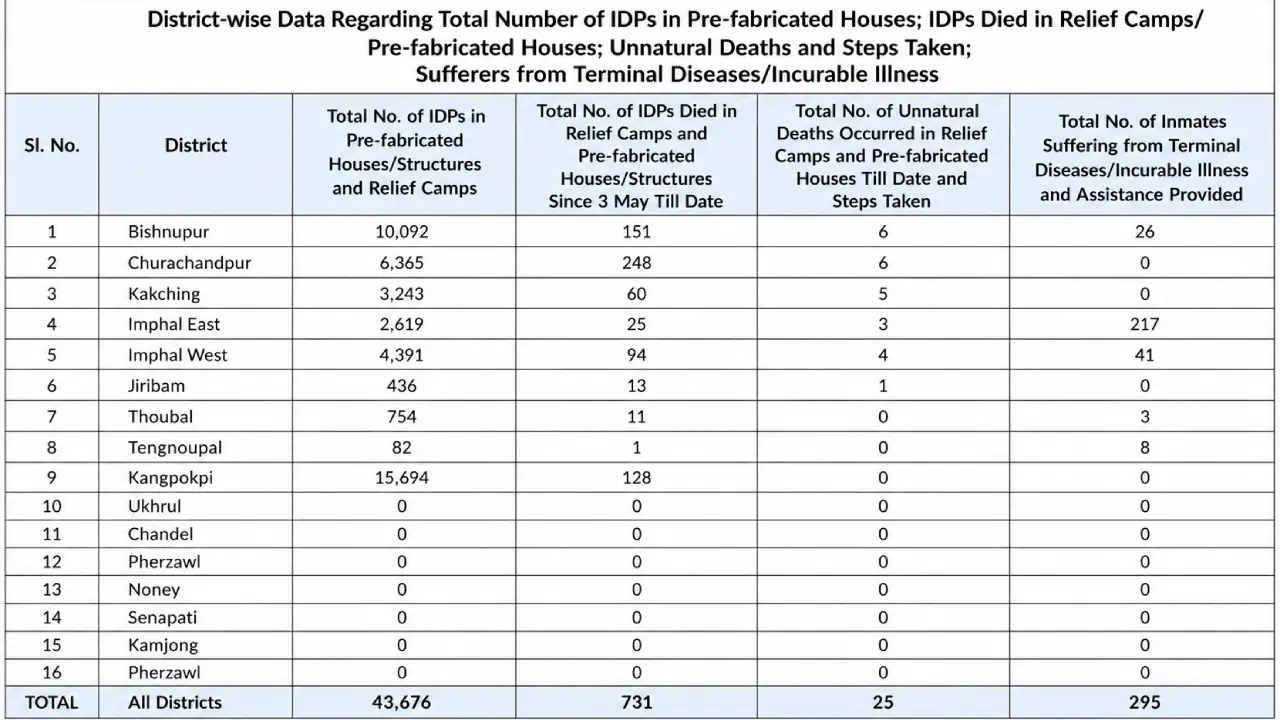
Kangpokpi is home to the largest concentration of IDPs: 15,694 people living in relief camps and pre-fabricated structures. It is followed by Bishnupur, with 10,092 — of whom 8,645 are in relief camps and 1,447 in pre-fabricated housing built to accommodate longer stays. Churachandpur records 6,365 IDPs as of April 30, 2026. Together, these three districts account for more than 32,000 of the total displaced population — roughly three-quarters of everyone captured in the data.
The remaining districts taper off sharply. Imphal West has 4,391 IDPs; Kakching, 3,243; Imphal East, 2,619. Thoubal accounts for 754, Jiribam for 436. Tengnoupal is a peculiar case: only 82 people are formally registered as camper IDPs, but there are 1,208 non-camper IDPs in the district — people displaced by the same crisis who are living entirely outside the official relief infrastructure, with no guaranteed access to the health monitoring or material support that camp residents receive.
At the other end of the spectrum, six districts — Ukhrul, Chandel, Pherzawl, Noney, Senapati, and Kamjong — reported no relief camps at all. Whether this reflects an absence of displacement, community-level absorption, or simply an absence of formal documentation is not addressed by the data. What it does confirm is that the administrative burden of this crisis falls almost entirely on a narrow geographic corridor while the rest of the state has been largely spared institutional disruption.
731 Deaths: The Mortality Record
Of the 731 deaths recorded since May 3, 2023, the heaviest toll has fallen on Churachandpur and Bishnupur.
Churachandpur has recorded 248 deaths — the highest of any district. Bishnupur follows with 151. Kangpokpi, despite having the largest IDP population, reports 128 deaths. Imphal West has recorded 94, Kakching 60, Imphal East 25, Jiribam 13, Thoubal 11, and Tengnoupal one.
The data classifies 25 of these as unnatural deaths. The rest — more than 700 — fall into a category the government records as natural deaths, covering illness, age, and causes consistent with the chronic health pressures of prolonged camp life. The data does not disaggregate this further. What exactly the 706 natural deaths consist of — how many were preventable, how many were exacerbated by camp conditions, how many were elderly, how many were children — is not disclosed. The number sits in the record without further explanation.
Unnatural Deaths: A District-by-District Account
The 25 unnatural deaths are documented in some detail, and the picture they present is one of varied but recurring hazards.
Churachandpur recorded six. Four people drowned. One died by electrocution. One was a victim of sexual assault; the accused has since been arrested and the victim's family received counselling through a One Stop Centre.
Bishnupur also recorded six, split between pre-fabricated housing and relief camps. The data does not specify the nature of each death but confirms they span both types of displacement settlement.
Kakching recorded five unnatural deaths — one drowning and four road accidents. The proximity of camp locations to roadways and the lack of formal traffic barriers around temporary settlements are known safety gaps in displacement sites. These numbers put them on record.
Imphal West had four: two cases of hanging, one drug overdose, and one bullet injury. These deaths — suicides and violence occurring within or near a displacement site — are the sharpest indicator of the psychological conditions facing long-term IDPs. Three years of camp life, uncertainty about return, and proximity to an unresolved conflict have left visible marks on the mental health of the displaced population.
Jiribam recorded one unnatural death. Kangpokpi and Thoubal reported none.
Terminal Illness: The Silent Health Emergency
Perhaps the most arresting number in the entire disclosure is from Imphal East: 217 camp inmates are recorded as suffering from terminal or incurable illnesses.
This is not a district with a large IDP population — Imphal East has only 2,619 registered IDPs, less than a fifth of Kangpokpi's total. Yet it carries by far the heaviest burden of terminal illness. What that means in practice — how many of these individuals can access specialist care, how many require palliative support, how many have family members able to accompany them to referrals — is not laid out in the data. But the figure alone is significant enough to demand attention.
Imphal West follows with 41 terminal or incurable cases among its 4,391 IDPs. Bishnupur records 26, and Thoubal three. Kangpokpi — the district with the single largest IDP population in the state — submitted that this information remains with the Chief Medical Officer and has not yet been included in the formal disclosure. Churachandpur and Kakching reported none.
Tengnoupal presents a different profile. Its small camp population of 82 residents includes three people with hypertension, four with diabetes, and one with chronic asthma — conditions that require consistent medication and monitoring. In a temporary settlement without a permanent pharmacy or reliable supply chain, managing these diseases over months and years is not straightforward.
What the Health Response Actually Looks Like
The quality and nature of medical support varies considerably from district to district, and the data gives enough detail to illustrate the gaps.
Imphal East operates what the data describes as a bi-weekly model — Medical Officers visit twice a week, covering medicine, obstetrics and gynaecology, and ENT. Ante-natal care and immunisation are also provided within the camp system. Cases requiring advanced intervention are referred to RIMS or JNIMS. This is the most structured model described in the submission.
Thoubal has moved toward chronic disease management. The district is supplying specific medications: Amlodipine 5mg combined with Telmisartan 40mg for hypertension, Metformin 500mg combined with Glimepiride 2mg for diabetes, and Alphaketoanalogue for chronic kidney disease patients. The precision here — actual drug names and dosages — is a marker of how seriously the district has had to take the long-term nature of this emergency.
Bishnupur has activated the District Mental Health Programme team, which operates with consultant psychiatrists, clinical psychologists, and psychiatric social workers. The records indicate that following unnatural deaths in the camps, the team provided immediate counselling and group support to bereaved families. This is a reactive model — mental health services deployed in the aftermath of suicide or drowning, rather than as routine camp support. That it is documented as a response to specific deaths gives an indication of how far conditions in some camps have deteriorated.
Jiribam handles cases through its One Stop Centre and the District Child Protection Officer. The approach addresses both individual crisis counselling and child-specific protection needs within the camp population.
Kangpokpi, with the most IDPs, provides only a general note in the submission — that medical relief is being provided and that specific health data remains with the CMO. This is the district where the data is thinnest, for the population that is largest.
Financial Outlays for Individual Care
Among the more unusual details in the disclosure is the level of specificity with which Imphal West reported financial assistance to individual IDPs requiring medical care.
Named beneficiaries received direct financial sanctions: Rs 98,750 was sanctioned for the surgery of Kh. Binasakhi Devi; Rs 89,296 for the son of L. Biren Singh for a surgical procedure; Rs 20,000 for Thongbam Keina for keyhole surgery. These are not large amounts relative to the cost of medical procedures, but they represent formal government acknowledgment of individual medical need and some degree of administrative follow-through.
Equipment procurement has also been recorded. Rs 68,900 was sanctioned for 13 air mattresses — essential for bedridden patients or those with pressure sores, common in camp populations with limited mobility. Rs 1,80,003 was allocated for medicines and wheelchairs. A further Rs 5,91,326 was sanctioned for a combined purchase of medicines and air mattresses.
Many IDPs across districts hold CMHT (Chief Minister's-gi Hakshelgi Tengbang) or Ayushman Bharat (PMJAY) cards, which provide a basis for government-covered health expenditure at empanelled hospitals. The extent to which these cards are actually usable — given displacement, documentation challenges, and the practicalities of reaching empanelled facilities — is not examined in the submission.
How the Data Was Obtained
This disclosure did not come through routine government reporting. It came through persistent legal action.
Goshwami's original RTI application was filed on September 8, 2025. It was not answered. He filed a second appeal. The Manipur Information Commission took up the matter and on April 21, 2026 issued a specific direction requiring the SPIO — the Joint Secretary (Home) — to furnish consolidated, state-level IDP data.
The Commission held a hearing on June 4. At that hearing, Shri Simon Loitongbam, representing the SPIO, tendered an unconditional apology for the delay, citing a shortage of time for gathering information from district-level offices. Even at that late stage, data for Imphal West and Chandel had not been received. The Commission noted the deficiency on record.
The following day — June 5 — Joint Secretary Moirangthem Kapajit Singh filed the completed information. Imphal West data was included. Chandel, which reported no relief camps, remained a formal gap in the submission.
Nine months from first application to final compliance. That is the timeline it took for a citizen to obtain information about a humanitarian crisis unfolding inside his own state — a state where tens of thousands of people are living in pre-fabricated houses, where hundreds have died, and where 217 people in one district alone are listed as terminally ill.
What the Data Does and Does Not Tell Us
The disclosure is significant precisely because nothing comparable has been made available through ordinary government communication. For three years, the IDP population in Manipur has existed largely as a political backdrop to a conflict that has attracted international attention but produced limited administrative transparency.
What this data confirms is the scale, the distribution, the mortality record, and the outlines of a public health burden. What it does not resolve is any of the harder questions: the condition of the 706 people who died of natural causes in displacement, the situation of the more than 1,200 non-campers in Tengnoupal who live entirely outside the documented system, or the long-term trajectory for any of the 43,000 people who remain displaced three years after May 3, 2023.
The Manipur Information Commission — through a single RTI appeal — extracted more usable data on this crisis than three years of official statements had produced. That should be read as a comment both on what the RTI Act can achieve and on what ordinary government accountability has failed to deliver.